The knock of the knot – Breast Cancer with a Lacanian Shape Angle Curve
The Real – Fear Intrigue Fortitude
Deride me not when I write sous rature! Part of my kick is the satisfaction achieved in the toying with language. Or even the loy of tanguage: tangle, wrangle, engage, joy, toy, employ. This chapter traverses the path between the lumpectomy and its clinical findings. The chapter examines jouissance and the Lacanian Symptom in a manner that endeavours to simplify their guises. It questions how much control each of us has over our own health. Could you rot an apple with your mind? The final paragraph situates the patient face to face with the oncologists’ verdict on a day when other distracting matters took the cancer pedal off the gas!
Derrida’s first indebtedness to Heidegger lies in his use of the notion of sous rature (‘under erasure’). To write ‘Under Erasure’ is to write a word, cross it out, and then print both word and deletion. Visually the original word may be read and understood alongside its replacement. Once it has been crossed out, it is barred, its relevance is questioned. It is erased but still shows evidence of a path once taken. How does what it meant before compare with its meaning now? Meaning can be inferred in a transference from the symbolic of the writer into the personal imaginary of the reader. The reader already has a mille-feuille of layered of meanings to wrangle with. How does writing “sous rature” add to the multitude of signifiers that vie for a priority of meaning?
Angles Curves Straights From Something to Something Else
Breast surgery leaves a woman with cuts and scars: period. We do not know what will become of us when this journey begins. Surgeons hope for the best outcome but healing is individual. As these marks heal, some rise and wheal, some turn into thin, flat, silver slivers, others redder, wider jaggedness. Under the skin the flesh has been torn. This seismic movement may leave lumps, bumps or oddly smooths – more straights than curves, or more bulges than straights. How our bodies are left will never be static, always evolving. Our states will never be still: our mornings different to our evenings and our hormoanal tides, wild or tamed will shift the balance.
Jouissance
Jouissance is both how we feel and react to our inner drive to enjoy ourselves. Jouissance is our individually chosen “carpe diem” how we choose to seize the day. In their chapter metapsychology: from body to history, Bazan and Detandt (2013) propose that jouissance is in the order of “agieren” or taking action. In this sense the pleasure is felt more strongly in the action leading to the seeking of an object of desire than actually obtaining that desired object. They suggest that jouissance is related to the release of motor tension that brings relief to the drive. While pleasure implies the consumption or attainment of an object (objet petit a) jouissance is in the use of the body.
The Symptom
How we deal with life, particularly within the time of an evolving cancer journey depends on our calling, our ego and how we choose to channel the release of our libidinal drives. The Lacanian symptom is the way in which we pursue our jouissance. The symptom may take the form of a character trait, manifested as being over tidy or untidy, controlling of others or being subservient. It may compell us to seek solitude or reacquaint with friends. Seek wide outdoor spaces or stick to homely routines. It may take an artistic form. Often anxiety and the libido transformed in crisis becomes the organizing principle of the jouissance of the artist or writer. Thus our mode of jouissance is the Lacanian symptom. Our particular chosen activity and our way of enjoying it will be repeated. This is because it gives us each, (as the human subject) a consistency. Our chosen “passion” is part of who we are. The Lacanian symptom is the visible trace of the particular modality for the subject’s jouissance. It is how the subject takes action to manage the distracting, disruptive, destructive, flotsam-jetsam of the unconscious. Jouissance is about how we silence, quieten or use-up our internal individualised libidinal chitter-chatter. It is how we tame this unconscious background noise of the mind, whose volume is often ten fold when faced with an uninterpretable Real: cancer.
Jouïs-sens (to hear meaning) Jouis-sens (to enjoy meaning)
The Real is the yet unsymbolised. It often looms up alongside a life changing event: a bereavement, an illness, a trauma, a cancer diagnosis. It often brings us in touch with our mortality and the ephemerality of life. This dance around the Real is an unconscious delving into our unconscious, stirring of our fears, fuelling and symbolising our imaginings, whilst relentlessly giving no respite. There is no escape from the Real. It catches us unawares from an angle seen awry. It is a sudden recognition of something unrecognisable. This misrecognition, a méconnaissance is where the subject becomes alienated in language, adrift beyond the symbolic, beyond expressible description. The impenetrable le mur du langage “wall of language” leaves the unnamed Real of the unconscious entrapped. The unnamed essence that is the unconscious will haunt us even more persistently in sleep. Sleep, where in our dreams anything goes. Where contradictions unify and nothing is prohibited because there is no “no” in our dreams. The unconscious is independent of language, a place where no meaning has been inscribed. In psychoanalysis however, unconscious meaning may move to the dominion of the preconscious, awaiting the intermediary of language. (J)ouïs is taken from ouïr to “hear” as the analyst listens. Progressively the analysis takes form through a matter of suturing and splicing until meaning is heard, jouïs-sens (to hear the sense or meaning). The desired psychoanalytic outcome being: Jouis-sens – I enjoy, I make sense – Enjoy-meant!
In Écrits, “Psychoanalysis and its Teachings” Lacan views the symptom as inscribed in a writing process. The symptom is a pure jouissance addressed to no-one because it is the manifestation of the way a subject enjoys (jouit) their unconscious, (Seminar “L’angoisse” 1962-63). Creative outlets during times of crises are undertaken for their own sake, if others can be appreciative then all well and good, but in the first instant they are a release, a way to channel the raw libidinal energies of the bodily drives. Creative outlets are a way to deal with the un-symbolised unconscious as the Real seeks a translation. The Real clamours to be symbolised with its “compelling and potentially horrifying alien material persistence” (Žižek 1997: 55–106; Braunstein 2003; Declercq 2004). It demands an outlet as it squeezes through the register of the Imaginary. Perhaps eventually it may succumb to a conscious translation in the more manageable symbolic realm. Although primarily the traumatic material of the Real is unsymbolised knowledge which nags submerged. It is latent, only occasionally rising (often with anxiety) as knots in our language and thought.
When Jean Hyppolite asks: “What use does the Symbolic have?” Lacan answers: “The Symbolic, the Imaginary and the Real are useful in giving its meaning to a particularly pure symbolic experience, that of analysis.” Since the symbolic dimension is the only dimension that cures, “The symbolic order is simultaneously non-being and insisting to be, that is what Freud has in mind when he talks about the death instinct as being what is most fundamental: a symbolic order in travail, in the process of coming, insisting in being realised.” Thus the “conquest of the symbolic order is essential for the human being to accede to a humanized structure of the real.” (S3 p.198).
Lacan was fond of saying “the Real is impossible,” impossible in that we cannot express it in language because the very entrance into language marks our irrevocable separation from the Real. Nevertheless in the event of acknowledging the materiality of our existence the Real overwhelms us. It forces a recognition that is perceived as traumatic as it punctures and threatens our very “reality” and drives us toward Lacan’s sense of jouissance.
Repetition and Joui-Sans
In Lacan’s later period he maintained that our methods of jouissance facilitate an achievement of libidinal-consistency by expressing-out our anxiety-evoking encounters with loss and lack. Through jouissantesque activities the holes that burrow into the pain of the Real are explored. During this (artistic, therapeutic or psychoanalytic exploration) unspeakable materials may begin to be brought to light symbolically, rather than being felt as psychogenic and enigmatic somatisations. The symptom is brought to the fore through repetition. In repetition we seek to recapture the first thrill of jouissance. Yet repetition is the curious link between the pleasure principle aka jouissance and the hidden mask of the death drive that is camouflaged behind this joy. Pleasure turns to displeasure as there is no recapturing the intensity of the very first instance of pleasure. There is no repeating the depths of ecstasy felt for the first creation, achievement or mastery. The death drive encroaches and its shadow looms larger in sync with the momentum of repetition. Pleasure turns to displeasure and eventually pain because repetition dilutes and slowly annuls the initial thrill into a consistency and evenness. There is no way to re-live the first hit of joy because everything after the first “buzz” is a reminder, a reminiscence, a substitute which never-quite has the real authenticity of the first time. If the pleasure endures, there is only so much pleasure one can take before it becomes painful pleasure. Thus jouissance is suffering, (S7, 184). Our jouissance mutates toward the frustration of an embittering joui-sans. For an interesting article see Bazan and Detandt (2013) http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3818686/
Home after the lumpectomy
Home, but wounded again. Just as my body had completely recovered from the biopsy the proper surgery was done already. For weeks the biopsy aftermath had continued to zap its zings of nerve healing pain. The pain wasn’t immediate but began a week after the intervention. It was a deep abrupt “high pitched” pain arriving with no warning. Now home after the lumpectomy I was facing another state of external and internal disrepair. It was a place of limbo with no health certainties. Thrown back into a strange day-to-day without yet having a medical verdict. Hemmed in by the hourly “what if” thoughts: If the cells had spread to the lymph my prognosis would alter. The incision was below the arm pit. It was hidden, covered by a large square of gauze and a wedge of waterproof bandage. Ablutions followed post surgery care instructions. It would withstand a soft daily shower but not a baptism of emersion. I tended it cautiously. A trickle of water poured like a delicate vintage. Whilst feeling more brazen with the healthy good-side, I was more todo-terrano, enjoying the normality for functional manhandling: relishing a one-sided hot shower and the rougher texture of a dry towel.
Exercises for post surgery breast healing
I felt sad for my condemned pampered breast. Would it prove to be innocent or a traitorous accomplice harbouring the most evil malignancy? The bandage strips were strapped up tightly to give decent support all day and the maternity bra was helpful and comfortable to sleep in. It’s amazing how the body fixes itself. Every day it felt a little better. I continued to maintain the stretch exercises by using the routine sheet I’d been given to prevent stiffness. The first stages of limbering were standing poses. Reaching my arms up, stretching higher each day. The tissue tension was most noticed in the Winging It exercise. Placing hands behind the head, with elbows askew and gradually brought inwards to touch. Then the same but lying down: hands behind head and bringing elbows to touch, then lowering them to the floor. Ouchy, now that stretch was trickier! At first it was impossible to push my arms to the floor. The skin was taut and tight, but slowly over days it improved.
Then the same but lying down: hands behind head and bringing elbows to touch, then lowering them to the floor. Ouchy, now that stretch was trickier! At first it was impossible to push my arms to the floor. The skin was taut and tight, but slowly over days it improved. 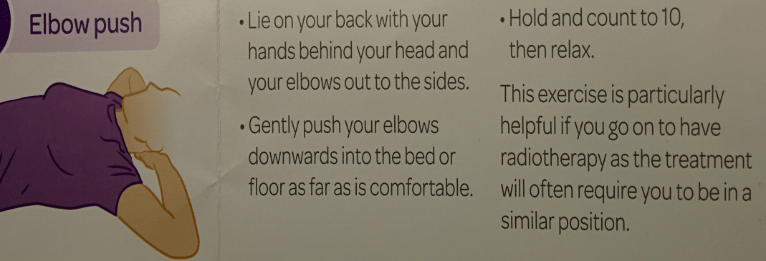 Then a particular standing stretch I’d discovered (which wasn’t on the instruction sheet) was also incredibly hard: bringing the arm on the injured side across. Holding the right arm (of the injured side) out stretched to the right then bringing it ahead and then diagonally across the body to the left. What a tug to the back muscles that caused!
Then a particular standing stretch I’d discovered (which wasn’t on the instruction sheet) was also incredibly hard: bringing the arm on the injured side across. Holding the right arm (of the injured side) out stretched to the right then bringing it ahead and then diagonally across the body to the left. What a tug to the back muscles that caused!
Comforting Accessories
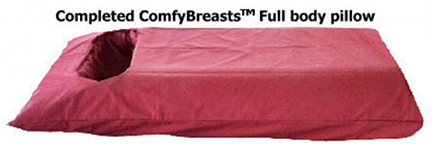 Sleeping was difficult. My dream idea was a mattress designed with a chest slot similar to the above. I didn’t go for this but would be interested in hearing of its efficacy. After the surgery my preferred position, sleeping face down, was on-hold indefinitely. To be pain-free the injured side needed to be maintained parallel. Not so easy to keep the breast aligned on top. It helped to prop a pillow along the side of my body adjacent to the breast, to keep it from sinking to the side. The parallel arm slightly elevated. I found a site with some interesting breast pillows but following surgery I didn’t find them useful.
Sleeping was difficult. My dream idea was a mattress designed with a chest slot similar to the above. I didn’t go for this but would be interested in hearing of its efficacy. After the surgery my preferred position, sleeping face down, was on-hold indefinitely. To be pain-free the injured side needed to be maintained parallel. Not so easy to keep the breast aligned on top. It helped to prop a pillow along the side of my body adjacent to the breast, to keep it from sinking to the side. The parallel arm slightly elevated. I found a site with some interesting breast pillows but following surgery I didn’t find them useful.
http://breastcancer.about.com/od/treatmentoptions/tp/comfort_pillows.htm
Power of Thought – Healing v Harming
A ten day wait lay ahead. What would the outcome be? The ideal scenario would show clear margins with no lymph involvement. But thought power was not going to change the verdict. You can’t seriously wish yourself well or think yourself sick…can you? I tried not to let my mind wander through the consequences. But around this time there was an article that created a bit of a furore. It was about the power of positive versus negative thinking.  Brow furrowed and lips pursed in thought. Can you rot an apple more quickly by throwing it a barrage of hateful thoughts. Well apparently so. Everyone would agree that you can’t wish yourself to win the lottery. You can’t really create a voodoo-like hex to wish ill on yourself or indeed others. Wishful thinking is surely as it sounds: wishful. A timely article indeed to show the power of scepticism and how a damaging mind-set supposedly causes actual bodily harm.
Brow furrowed and lips pursed in thought. Can you rot an apple more quickly by throwing it a barrage of hateful thoughts. Well apparently so. Everyone would agree that you can’t wish yourself to win the lottery. You can’t really create a voodoo-like hex to wish ill on yourself or indeed others. Wishful thinking is surely as it sounds: wishful. A timely article indeed to show the power of scepticism and how a damaging mind-set supposedly causes actual bodily harm.
http://thecharismamodel.com/the-big-apple-experiment-gallery/
Bewilderment – Be Wilder I Meant!
So the “C” diagnosis is a long fall down. Hitting the ground takes longer than you may think, with some of us hanging on before falling further. The diagnosis leaves survivors in a minefield of bewilderment. Now this is a word for a little Lacanian mischief. A word that states it is “meant” to “be” “wilder”. In this wilderness one is left to roam, to be separated, estranged, isolated, from the logical sense and meaning of “the other”. In this wilderness the patient may forget the symbolism of what is said or read. Instead being left to tune in to the body, filtering-away the white-noise of the outside. Instead listening to an imaginary dialogue of a future yet to be lived. Pre-diagnosis leaves the mind to wander and wonder. The realm of the wandering leaves us wondering where the next trip wire may be.
Echoes of you’ll be fine, they’ll figure it out are reassurances from the “big Other” – hopeful sound bites used as part of the illness language schema. So I wait, impotent and expectant, silently numbing scepticisms of any half empty glass. How will one accept and cope if faced with a sorry verdict. It is my body. If it is rotten at its core it will still be my body. Things could still swing back to the knife. Further slices required if there weren’t clear margins. If the lymph were to be affected then all sorts of possibilities open in the road ahead. Iffing and butting are impossible to surpress and they help the psyche prepare.
Word and Action
Ten days after the surgery the essential appointment arrived. My mind wasn’t actually tuned in. The admissions secretary assured us (I wasn’t alone) that my early appointment was not running late. My preoccupation was distracting. I needed to be seen to have the healing process checked. Beyond that it was all ce la vie. An automaton, I needed to leave. My eyes were darting to the time. The door opened punctually at 10am. How efficient would this be? Entering the clinical room, the dressings were removed, the red-rawness of the scar was positively appraised and the skin-tissues were left to support themselves. In preparation, my underwear seams had been cut away to leave room for the bare skin. All was repairing nicely. We had a train to catch. My mind was not on my situation. We had to leave this appointment and leggit to the station. We couldn’t miss the train and arrive late. A week after my lumpectomy operation, my step-sister had been ingressed into a hospice. She had barely arrived there before passing away from stage 4 breast cancer. Two years earlier her symptoms had been leg and back pains and her prognosis the most grim. My appointment was at ten and her funeral, fifty miles from London was four hours later. Dressed once again we were escorted to hear my verdict. What had the surgeon found? We jostled into a tiny room with three oncologists preparing to tell the news. Hear it and run was the voice in my head. It was good news. The best news: low grade, small area of cells (<15mm) clear margins and no sign of trespass to the lymph. I didn’t want to stay to negotiate my treatment. Deep inside, I knew that they would follow the clinical protocol. Even if I had questions the “treatment package” was set in stone. Right now I had to leave. Perhaps they’d expected a bit more of a battle from me or at least a barrage of my usual questions. My chair scraped the floor as I pushed back and arose to gather my coat. We must have cut a strange silhouette in our angular black funeral attire. We barely shook hands before pelting out into the street to pay our respects to someone who’d been dealt a harsher hand and was waiting for her final farewell.


 The surgical team watch as the dye collects in the first lymph nodes. This process of
The surgical team watch as the dye collects in the first lymph nodes. This process of








{kind=link}